CASE REPORT |
https://doi.org/10.5005/jp-journals-10001-1548 |
A Case of Temporal Bone Erosion: Our Diagnostic Dilemma
1,2Department of ENT, Jeevika Hospital, Bengaluru, Karnataka, India
Corresponding Author: Amrita Suzanne Mathew, Department of ENT, Jeevika Hospital, Bengaluru, Karnataka, India, Phone: +91 7337876356, e-mail: amritasmathew@gmail.com
Received on: 01 March 2022; Accepted on: 09 January 2023; Published on: 21 February 2023
ABSTRACT
Background: Cholesteatoma is a sac containing keratin debris surrounded by keratinized squamous epithelium with bone-eroding properties. Secondary cholesteatoma is the commonest type of cholesteatoma. Middle ear cleft cholesterol granulomas (CG) usually present with middle ear effusion and features of diffuse mastoid disease. Hemorrhage, drainage obstruction, and impaired ventilation precipitate CG formation. The latter two factors also contribute to the pathogenesis of chronic otitis media (COM) and cholesteatoma, often leading to their coexistence. CGs are rarely aggressive and are encased by thick fibrous tissue with bone-eroding capabilities. However, differentiation of a cholesteatoma from a CG based on computerized tomography (CT) is difficult and necessitates magnetic resonance imaging.
Case description: We report a rare case of a secondary cholesteatoma with a coexistent erosive tympanomastoid CG causing erosion of the basal turn of the cochlea but with an intact scutum, thereby presenting a diagnostic challenge.
Conclusion: Evidence of bone erosion on a computerized tomogram in patients with COM does not indicate the mere presence of a cholesteatoma. A differential diagnosis which includes other erosive conditions such as glomus tympanicum, CG, etc., which can coexist with a cholesteatoma, should be considered and investigated accordingly in order to plan its surgical treatment.
How to cite this article: Shilpa H, Mathew AS. A Case of Temporal Bone Erosion: Our Diagnostic Dilemma. Int J Head Neck Surg 2023;14(1):13-15.
Source of support: Nil
Conflict of interest: None
Keywords: Acquired cholesteatoma, Cholesterol granuloma, Temporal bone.
INTRODUCTION
The presence of CG is often an associated finding in patients with COM, particularly those with cholesteatoma.1 Otic capsule invasion by CG is rare, presenting a diagnostic challenge to otologists and radiologists due to the inability to differentiate a cholesteatoma from a CG on CT.2
Though cholesteatomas are characterized by a soft tissue density in the mesotympanum/epitympanum or antrum, high-resolution CT (HRCT) temporal bone is unreliable in the differentiation of various soft tissue/fluid densities. With scutum erosion being the earliest definitive sign of a cholesteatoma, bone erosion is a requisite radiologic sign of a cholesteatoma, the absence of which precludes its definitive diagnosis.3
Glomus tympanicum (a slow-growing, locally invasive tumor) is the commonest lesion over the promontory. CT demonstrates an enhancing myalgic encephalomyelitis (ME) soft tissue density lesion, with the erosion of the basal turn of the cochlea but sparing the ossicles.4
Both cholesteatoma and CG of the ME and mastoid may cause intratemporal, and intracranial complications. Thus, early detection and treatment are crucial.5 We, therefore, report a rare case of a secondary cholesteatoma with an erosive ME, CG, with the erosion of the basal turn of the cochlea but an intact scutum, thereby presenting a diagnostic dilemma.
CASE DESCRIPTION
A 55-year-old male presented to the Department of Otorhinolaryngology with left ear discharge and decreased hearing for 12 years. Discharge was episodic, profuse, mucopurulent, nonfoul smelling, and nonblood stained but became continuous, scanty, watery, foul smelling, and blood stained for the past 2 years. Otoscopy revealed a granulation polyp in the posterosuperior quadrant of pars tensa, with a normal attic.
High-resolution CT (HRCT) revealed soft tissue density in the epitympanum and mesotympanum extending into the antrum with a sclerotic mastoid. Erosion of the long process of the incus and tympanic segment of the facial canal was seen. However, a peculiarity noted was the erosion of the basal turn of the cochlea, with the outer attic wall remaining unaffected. Planning of appropriate surgical intervention necessitated contrast-enhanced CT (CECT) to rule out a glomus tympanicum (the commonest cause for erosion of the cochlear promontory). The lesion was nonenhancing with contrast administration, thereby ruling out a glomus tumor (Fig. 1).
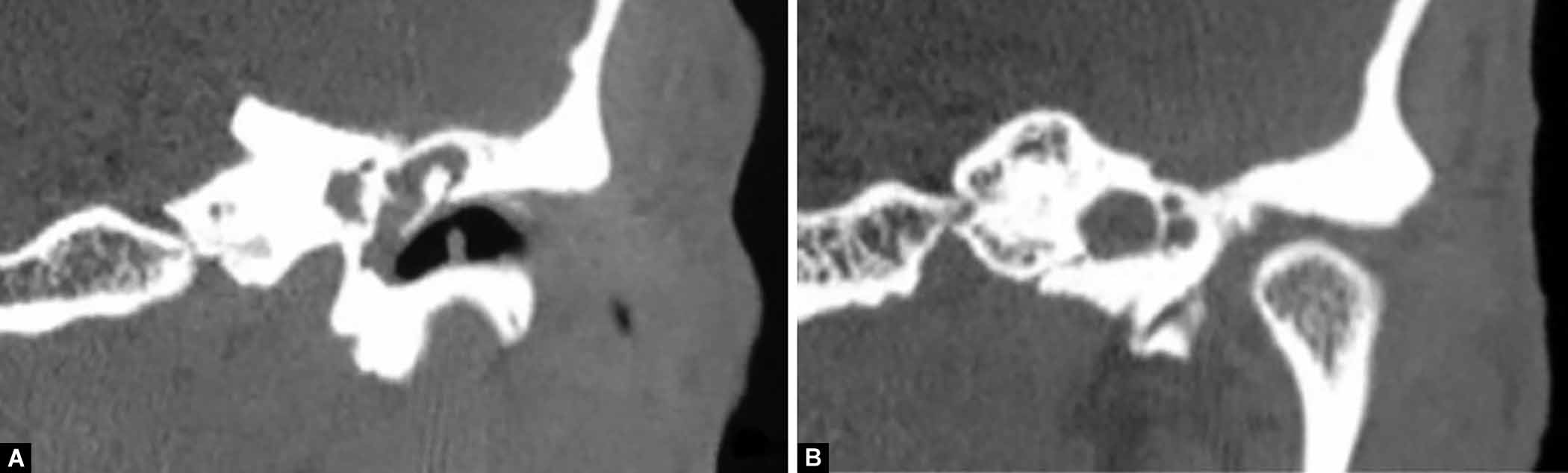
Figs 1A and B: HRCT temporal bone coronal images. (A) Soft tissue density in the left middle ear with intact scutum; (B) Erosion of left cochlear promontory
Pure tone audiometry showed 66 dB mixed hearing loss in the affected ear with a 30 dB air-bone gap. With the diagnosis of a cholesteatoma, we proceeded with mastoid exploration. Intraoperatively, a CG was noted in the promontory region (confirmed histopathologically). CG and granulation tissue were excised in toto. On opening the antrum, cholesteatoma was noted involving the antrum, extending into the anterior epitympanum (Fig. 2). Modified radical mastoidectomy (MRM) with type 3 tympanoplasty and ossiculoplasty using sculpted nasal septal cartilage from our cartilage bank, was performed. Postoperative follow-up was satisfactory.

Figs 2A to C: (A) Intraoperative picture showing a mass arising from middle ear–? Cholesterol granuloma; (B) Cholesteatoma visualized on opening the antrum; (C) Histopathological study of mass excised from middle ear confirming a cholesterol granuloma
DISCUSSION
Cholesterol granulomas (CG) of the temporal bone are expansile, thickly encapsulated, cholesterol-containing cysts surrounded by chronic inflammatory foreign body giant cells. It is most likely a foreign body reaction to blood and blood breakdown by products.2
There are two forms of CG—aggressive petrous apex CGs and the common, nonaggressive tympanomastoid CGs. Tympanomastoid CG can occur in the ME cleft in conjunction with COM/mastoiditis in patients with transverse myelitis (TM) perforation (as seen in our case), or in the absence of infection, behind an intact TM.1 The obstruction vacuum theory explains the formation of temporal bone CGs.6 CGs are possibly secondary to the cholesteatoma (i.e., ingrowth of keratinizing squamous epithelium into the ME/mastoid), which isolates and blocks off segments of the ME cleft.1
Aggressive/destructive tympanomastoid CGs are extremely rare (bone erosion and extension beyond the limits of the ME and mastoid i.e., invasion of the basal turn of the cochlea, middle, and posterior fossae dura, walls of the sigmoid sinus and carotid artery, etc.).5 A relationship between these lesions and highly vascular sources has been found.6 Bleeding from these vascular sources has been hypothesized to provide the trigger for the morphogenesis of CG, thereby explaining their aggressive nature.7 In our case, contiguity was noted between the erosive CG and granulation polyp.
Cholesteatomas are channeled along characteristic pathways, commonly located in the posterior attic, posterior mesotympanum, and anterior attic.8 Incus is the most commonly eroded ossicle identified on CT in 92% of cases.9 Although CT cannot distinguish soft tissue from effusion or granulation, or granuloma in patients with attic cholesteatoma, erosion of the scutum, which is the first sign of cholesteatoma, can be assessed clearly.8 The absence of outer attic wall erosion, along with the finding of erosion of the cochlear promontory and ME cleft soft tissue, led us to further investigate our case.
The cochlear promontory is the site for lesions such as glomus tympanicum, congenital cholesteatoma, and Jacobson’s nerve schwannoma, of which the first is the most commonest. Glomus tympanicum is a very rare, benign, slow-growing tumor of ME arising from the tympanic plexus over the promontory. It’s CT characteristics include an enhancing ME soft tissue density lesion, with frequent erosion of the basal turn of the cochlea, but with ossicular sparing, occasionally filling the ME cavity and extending into the external ear.4 However, our patient did not have pulsatile tinnitus or enhancement of the lesion on CECT, thereby excluding a glomus tumor.
Cholesterol granulomas (CG) are predominantly an incidental finding during surgical intervention for cholesteatoma/COM, as was seen in our case.6 However, achieving the goals of an ideal surgery, that is, a disease-free, normal-hearing ear with an intact TM and posterior canal wall, has been difficult. Although the hearing is slightly (but not significantly) better with the closed procedure than with the open procedures, a second procedure is often required when the closed method has been employed due to frequent occurrence of residual and/or recurrent disease.10 We, therefore, chose to proceed with MRM with type 3 tympanoplasty in our case, with satisfactory postoperative results.
CONCLUSION
Evidence of bone erosion on HRCT in patients with COM does not indicate the presence of a cholesteatoma. A differential diagnosis which includes other erosive conditions such as glomus tympanicum, CG, etc., which can coexist with a cholesteatoma, should be considered and investigated in order to plan its surgical treatment.
REFERENCES
1. Miglets AW, Booth JB. Cholesterol granuloma presenting as an isolated middle ear tumor. Laryngoscope 1981;91(3):401–405. DOI: 10.1288/00005537-198103000-00011
2. Mafee MF, Nozawa A. Primary and secondary cholesteatomas, cholesterol granuloma, and mucocele of the temporal bone: role of computed tomography and magnetic resonance imaging with emphasis on diffusion-weighted imaging. Operative techniques in Otolaryngology 2014;25(1):36–48. DOI: 10.1016/j.otot.2013.11.006
3. Yang NW. Blunting of the scutum: a key feature in the radiological diagnosis of acquired cholesteatoma. Phillipine J Otolaryngology–Head and Neck Surgery 2009;23(1):37–38. DOI: 10.32412/pjohns.v23i1.775
4. Raza SS, Hussain AK, Saboor H, et al. Glomus tympanicum tumor–A rare presentation in a tertiary care hospital of Peshawar. NJMS 2016;1(3):138–140. Available at: https://njms.pk/index.php/njms
5. Kuruma T, Tanigawa T, Uchida Y, et al. Large cholesterol granuloma of the middle ear eroding into the middle cranial fossa. Case reports in Otolaryngology 2017;2017:4793786. DOI: 10.1155/2017/4793786
6. Pfister MHP, Jackler RK, Kunda L. Aggressiveness in cholesterol granuloma of the temporal bone may be determined by the vigor of its blood source. Otol Neurotol 2007;28(2):232–235. DOI: 10.1097/MAO.0b013e31802bea4b
7. Iannella G, Stasolla A, Pasquariello B, et al. Tympanomastoid cholesterol granuloma: radiological and intraoperative findings of blood source connection. Eur Arch Otorhinolaryngol 2016;273(9):2395–2401. DOI: 10.1007/s00405-015-3820-5
8. Rogha M, Hashemi SM, Mokhtarinejad F, et al. Comparison of preoperative temporal bone CT with intraoperative findings in patients with cholesteatoma. Iranian J Otorhinolaryngology 2014;26(74):7–12. DOI: 10.22038/IJORL.2014.2020
9. Sharma VK, Prajapati N, Sharma R, et al. Radiological changes in anatomy of temporal bone in cases of unsafe chronic suppurative otitis media: a retrospective study. Indian J Otol 2017;23(3):176–179. DOI: 10.4103/indianjotol.INDIANJOTOL_15_17
10. Brown JS. A ten year statistical follow–up of 1142 consecutive cases of cholesteatoma: the closed vs. the open technique. The Laryngoscope 1982;92(4):390–396. DOI: 10.1288/00005537-198204000-00007
________________________
© The Author(s). 2023 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted use, distribution, and non-commercial reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.